Sometimes people go to great lengths to identify their dead even after many years of their disappearance.
In1995 8000 of Bosnian men and boys were murdered by the Serb troops led by Gen Ratko Mladic during the infamous war of partition of former Yugoslavia. The following is a paper clip showing the importance of identification of the disappeared even after 17 years for the relatives. (See - http://en.wikipedia.org/wiki/Srebrenica_massacre)
Slaughter without mercy, 17 years of agony and the day that 520 victims were finally laid to rest: Relatives sob as they bury men and boys massacred at Srebrenica
Read more: http://www.dailymail.co.uk/news/article-2172106/Srebrenica-massacre-Another-520-newly-identified-victims-laid-rest-mass-funeral.html#ixzz2Dd5n7NBn
Follow us: @MailOnline on Twitter | DailyMail on Facebook
Read more: http://www.dailymail.co.uk/news/article-2172106/Srebrenica-massacre-Another-520-newly-identified-victims-laid-rest-mass-funeral.html#ixzz2Dd5n7NBn
Follow us: @MailOnline on Twitter | DailyMail on Facebook
•Bodies of the victims are still being found throughout eastern Bosnia and identified through DNA analysis
•So far 5,325 Srebrenica massacre victims found have been laid to rest
•Thousands of Muslim men and boys were slaughtered in July 1995 by Serb troops led by Gen. RatkoMladic
• By Jill Reilly
PUBLISHED: 16:20 GMT, 11 July 2012 | UPDATED: 23:55 GMT, 11 July 2012 (Mail Online)
The identification of the dead for the information of the relatives on ethical and humanitarian grounds is only one reason why it is an essential part of a post-mortem examination.
The other reasons include;
1. For official, statistical and legal purposes
2. For the purposes of burial or cremation.
3. To discharge the legal obligations in relation to property, estate and debts
4. For the purposes of proving identity for life insurance, pensions and other financial matters
5. For the purposes of legal procedures such as trials, inquests and tribunals held by Inquirers, judges etc.
6. To facilitate the police investigations in to criminal or suspicious deaths.

Who is responsible for identification of human remains?
The police as the principal player of criminal investigation have the ultimate responsibility of identifying the human remains under investigation. For that they usually seek help from the forensic pathologist (JMO) and other relevant experts such as forensic anthropologists (expert in human bones), forensic dentist and forensic biologists (DNA).
Whenever a dead body or human skeletal remains are presented for autopsy it is the responsibility of the doctor to confirm the identification of the deceased before the dissection. This is usually done by inquiring the post mortem assistant, to whom the relatives have already identified the dead body. Other countries have different methods of dealing with such situations. If the doctor has any doubts about identification they should summon the relatives and verify the identification by themselves. Whenever the doctor goes to give evidence in the high court one of the first things the court asks is who had identified the body to them. Only in exceptional circumstances a dead body is dissected without proper identifications. This is usually the case in deaths of vagrants.
Principles of Identification
The objective of ‘identification’is to find out whose human remains are under investigation. It is basically to say that this is the remains of so and so. The process of identification can be divided into two phases. They may merge into to one in case of fresh human remains and remain separated in the case of skeletal remains.
Two phases of Identification are
1. General and 2. Specific
1. General Identification
Basically, in this phase human remains are assigned into a few general categories such as species (in the case of bones suspected to be of human), race, sex, stature and age. At the completion of this phase we would know the race, sex, stature and the age of the human remains. Buts still it does not produce a definite identification of the individual. This first phase is said to be based on ‘absolute’ criteria. They are called ‘absolute’ because examiner does not need any information about ante mortem data of a missing person to do this exercise. In other words, even if we do not have any idea who this person might be, nothing would prevent us from completing this phase of identification. At the end of the day we would be able to come up with certain information regarding the person, whose remains are under investigation. For example we would tell the police that the human remains belong to a woman of probably mongoloid race, between 18 and 25 years and 5’ 2” tall. By doing so the doctor helps the police to narrow the search for the missing person.
2. Specific Identification
This is often done after the general identification. Once the remains are assigned to a race and sex and estimated to be of certain stature and age the next phase, which is specific identification, can commence. (However, in most of the cases, these phases are done at the same time.)
In a practical scenario, the police might publish the information the doctor has provided about the general identification on news papers and the radio. The relatives, whose loved one has been missing for some time, might come forward to claim the remains as the general description given by the police matches those of their missing relative.
This is called specific as at the end of this phase the examiner should be able to identify the remains as belong to a particular individual. This is basically a comparative study matching the ante mortem data of a missing person with those of the remains under investigation. For example, a surgical prosthesis present in the remains is a good individualising feature of identification only if there is a missing person (of same race, age, sex and stature) who had exactly the similar prosthesis implanted before his/her death. Examples of specific identification features are:-
Facial identification
Clothes & ornaments
Scars, marks, tattoos, occupational stigmata
Bone diseases and trauma
Photo superimposition, facial reconstruction
DNA
Finger printing
Dental identification
These criteria of specific identification are divided into minor and major. The minor criteria include facial features, clothes & ornaments, scars, tattoos, marks and photo-superimposition etc. The major criteria include DNA, finger printing and dental identification.
Features useful in Identification
The availability of features useful in identification depends on the preservation of the body. They can be in various stages of decomposition. Some are mutilated and dismembered. A tattoo, very useful specific identification feature in a fresh or decomposed or mutilated body is of no use in skeletal remains. Therefore, the features, described below, may or may not be present in the human remains under investigations.
1. Facial Appearance
This is the most useful feature of identification in fresh bodies referred for medico-legal autopsy. Even if the body is in early state of decomposition it can be used for identification. However, it has been reported in the past that in some rare instances, relatives had taken a wrong body home thinking that it was the remains of their loved one.
Once facial features are distorted due to many post mortem factors such as rigor mortis, hypostasis, muscle flaccidity, flattening, etc. it is not easy to identify a dead body by facial features alone. Although we do not realise, most of the time identification by face involves not only its physical features but also its emotions such as smile, twinkling of eyes, wrinkling of forehead etc.
2. Eye colour, Skin Colour or Pigmentation and Hair Colour
They are not important features of identification in our part of the world as in the west unless the deceased was in the habit of colouring hair and wearing contact lenses of unusual colours.
3. Hair Structure
Examination of hair for the purpose of identification is a job of the forensic scientist.
Different racial groups have structurally different hair. Negroid head hair is dark having a spiral twist with a flattened, elliptical cross section. Mongoloid hair is less pigmented and straight with a cylindrical cross section. Caucasian hair is round or ovoid in cross-section.
Hair roots can be used to do blood grouping and other serological tests. They also can be used in DNA profiling.
4. Tattoos
They are produced by injecting coloured pigments under the epidermis using needles manually or with a vibrator. Although colours may disappear with the age the black pigment may persist lifelong.
They can be used both in specific and general identification.
Tattoos are much more popular in the west than in our part of the world. The labels attached to certain tattoos in the west for long time such as number 13 inside the lower lip in ‘drug pushers’, blue bird on the web between thumb and index finger in homosexuals are no longer valid due to the increased popularity of tattoos amongst the young. As a result value of them as a feature in general identification has waned.
However, it is still regarded as important ‘minor’ criteria of specific identification.
Photographing, recording and comparing tattoos for identification purpose are police duty. The doctor’s duty is to find them for the police if they are obscured. When the decomposition has set in tattoos may be covered under the loose skin. But when the skin is removed they can be vividly visible on the white dermis.
5. Finger, palm, foot and lip prints
The doctor need not know about how they are used in identification as they also come under police. However, they should know that all of them can be used in identification of individual depending on the availability. For instance, finger prints are not similar even between twins. The doctor’s role is limited to facilitate the police to take these prints in certain situations such as in decomposed bodies.
6. Scars
Scars of both surgical and other (accidental, self-inflicted or criminal) origins are important tools in identification. Some of the surgical scars such as appendicectomy and caesarean section scars may not be so specific as many members of public may have these scars. In contrast accidental, self-inflicted or criminally inflicted scars may be very useful in specific identification.
9. Occupational Stigmata
The specific markers of some occupations described in text books have declined in their importance e.g. blue scars in coal miners, pen callosities in clerks, shoe makers’ kyphosis. However, by examining the hands, the forensic pathologist can differentiate a manual worker from others, who engage in more sedentary work.
10. Stature of a body
There can be a difference on either way between ante mortem and post-mortem stature. Firstly it is not practically possible to take the exact measurement of length of a dead body due to various reasons. Secondly due to loss of muscle tone resulting from primary flaccidity, relaxation of large joints, loosening of inter-vertebral discs from the loss of tone of paraspinal muscles may increase the length by 2-3 cm.
11. Determination of sex in a non-skeletalized body
Most of the time external genitalia and secondary sexual characteristics would help to determine the sex. It may be difficult in extreme cases of transsexual who have undergone sex change surgery.
Circumcision may indicate the race and religion of the person.
Clothing and jewelleries may also help to determine the sex.
When the decomposition is advanced the presence of internal pelvic organs would help as the uterus and prostate are resistant to decomposition compared to other soft tissues and organs.
In skeletalized bodies the bones especially the pelvis and skull can be used in determination of sex. This will be dealt with later.
12. Age of non-skeletalized bodies
This is much more difficult than determination of sex. Greying of hair, loss of elasticity of skin with wrinkling and changes of tooth are not accurate methods to estimate age. ‘Arcus senilis’ may appear in persons who are more than 60 Years of age. More accurate methods will be discussed under the skeletal remains.
Identification of Skeletal Remains
Identification of skeletal remains needs expert knowledge in physical anthropology. Experts in radiology, dentistry, archaeology and DNA profiling may need to work as a team with the physical anthropologist. Therefore, examination and reporting on skeletal remains should always be done by the expert.
It should be noted that the expert’s view may be sought not only on complete skeletal remains but also on single pieces of item thought to be of a piece of a human bone. The approach to be followed in cases of skeletal remains in view of identification is as follows.
1. Are they bones?
2. Are they human?
3. What is the sex?
4. What is the Stature?
5. What is the Race?
6. What is the Age?
After allocating the skeletal remains into these categories of general identification the examiner can attempt to achieve specific identification using features specific to the skeleton under examination such as
1. Anatomical shapes (can be matched by radiology)
2. Frontal sinus comparison
3. Craniometry
4. Radiological bone architecture
5. Healing or healed fractures
6. Metal prosthesis
7. Bone diseases
8. Congenital defects
As the name implies this is an exercise of matching the ante mortem data with post-mortem data.
After achieving the identification of the remains, or sometimes even before that, the pathologist needs to answer two more important questions. They are:-
1. Time since death or disposal of body
2. The cause of death
Now we should see how to answer the following questions
1. Are they bones?
Although this seems to be a‘stupid’ question sometimes the police and the public being not trained in anthropology would bring pieces of various materials such as wood, plastic, stones etc to the pathologists suspecting that they are bones.
Shape, texture, weight, of the object would tell the pathologist they are not bones.
2. Are they human bones?
As long as the bones are intact the task is easy for the pathologist even if they are not trained in‘comparative’ anatomy. The size and shape of the bone usually indicate that they are not human. But in cases of small bones resembling human bones of the hands and feet and fragmented bones, especially long bones without ends, may pose a problem for the pathologist. In such cases a comparative anatomist with some forensic experience should be consulted.
One day, several years back we were told that a man had been murdered and dumped in a canal in Hunupitiya a few years ago. We went to the scene to see a ‘dredger’ was at work dredging the canal. After a few hours they found a black shopping bag with a tied mouth containing some bones. We took them to the department for examination. They revealed to be comprised of multiple small bones and scales. We suspected it was a ‘turtle’.Then we went thought the internet to do a bit of our own ‘comparative anatomy, which confirmed that it was in fact a turtle. Killing a turtle may be an offence under the Protection of Flora and Fauna Ordinance. But who would be prepared to spend time finding the culprit who killed the turtle in view of prosecuting him in a court of law?
Histology may help in distinguishing animals from human as they have different Haversian architecture. Serology, which would differentiate animal proteins from human protein, can help as long as extractable protein remains in the bones. Finally even the DNA can help in this endeavour.

Fig 01. The bone on the right looks like a femur but it is not obviously a human femur. Even if we may not be able to identify the animal we can definitely say it is not human. (This is probably a cattle bone).

Fig 02. What about these two? They both look like human hands don’t they? But the left is human and right is a bear paw. It is famously similar to the human hand. In this kind of a case the service of a comparative anatomist may be useful.
3. Determination of the sex
This is more important than estimation of age and stature as it approximately excludes half of the population.
The accuracy of determination of sex depends on the age, number of missing bones, degree of fragmentation and the biological variations.
It is common knowledge that the changes appear in the body after puberty. This is true for the bone development as well. It is obviously easy and more accurate to determine sex when the skeleton is complete. When the bones are fragmented it may be difficult to determine sex. Some of the features used for sexing the skeleton have biological variability.
This can be achieved in two different ways. The subjective way uses subjective assessment of certain bony features especially on pelvis, skull and long bones, which is also called‘osteology’. The objective ways uses measurements of the certain aspects of the bones to determine the sex which is also called ‘osteometry’.
For instance it is known that the femoral head is usually larger in males than in females. The researchers have found that femoral heads, which are more than a certain diameter, are more likely to be male.
The Skull
The features used in determination of sex are said to be valid only between 20 and 55 years as they develop after puberty and modify after senility. The most important features are:-
1. General Appearance
Female skull is rounder and smoother than the more rugged male skull.
2. Size – Male skull is larger with endocranial volume 200 ml greater.
3. Muscle Ridges more marked in male skull especially occipital area (nuchal lines) and temporal areas where the masseter and temporal muscles attached.
4. Supra-orbital ridges – more marked in male. Glabella is prominent in males and small and absent in females.
5. Mastoid process – larger in males
6. Palate – larger and U shape in males. Female palate tends to be parabolic
7. Orbits – are set lower and smaller in male. More square and less sharp edges than in female.
8. Forehead – high and steep in females with more rounded infantile contour than the male
9. Zygomatic process- the posterior ridge projects back beyond external auditory meatus in male. Zygomatic arches bow outward more than the female.
10. Mandible – larger in male with squarer symphysis. Female jaw more rounded and project less at the anterior point. Vertical height at symphysis is greater in males. Angle between the ramus and body is more acute in males being less than 125. Condyles are larger in male with broader ascending ramus and more prominent coronoid process.

Fig 03. This is a female skull. Look at the absence of supra-orbital ridges and glabella, small zygomatic arch and pointed chin. Forehead is smooth, rounded and not sloping.
Fig 04. This is a male skull. Look at the prominent supra-orbital ridges and glabella, thick and robust zygomatic arches and square chin.
Sex characteristics in pelvis
Unlike in the skull the features of sex differentiation are present even in the fetal pelvis. According to the experts sexing can be done using the pelvis alone with 95% confidence. The most important thing to remember is that these features should not be taken in isolation. What matters is the overall evaluation and not the single features. In some pelvis certain features may contradict each other.
General Appearance-The male pelvis is more rugged due to attachment of bigger muscles. It stands higher and more erect than smoother, flatter female pelvis.
Sub-pubic Angle- 900in female 700 in male.
Body of Pubic Bone- Triangular in male. Rectangular in female.
Pubic bone- In the female following can be present
‘Ventral arc’, a bony ridge running down the ventral surface from the pubic crest
‘Subpubic concavity’ – a concavity of the lower margin of the inferior pubic ramus
‘elevated bony ridge’ on the medial aspect of ischio-pubic ramus, immediately lateral to the symphysis (in the male this area is broad and round)
Acetabulum – larger in males. Faces more laterally in males. Antero-laterally in females.
Greater Sciatic notch –(important criterion) Deep and narrow in males. Wide and open in females.
Obturator foramen – ovoid in females. Triangular in males.
Preauricular Sulcus – on the pelvic bone just lateral to the sacro-iliac joint where the sacro-iliac ligament is attached. This is well-marked in females and absent in males.
Pelvic inlet – circular in female. Heart shape in male.

Fig 05. This is male pelvis. Look at the heart shape inlet and narrow sub-pubic angle. Sacrum has five segments.

Fig 06. This is female pelvis. Look at the round pelvic inlet and wide supubic angle.
Sex Characteristics in Sacrum
Female sacrum wide, short and has a shallow curve which is limited to distal part below the centre of the 3rdsacral vertebra.
Male may have more than 5 segments. The curve is continuous down to the whole bone and with forward projection of coccyx.
Sex characteristics of long bones
The femur is the best out of all the other long bones for sexing.
However, there is considerable overlap of all sex features in long bones.
Larger heavier bone with larger head is more likely to be male.
Since the pelvis is wider in females the femoral shaft has to slope more to converge at the knee level so that the condyles at the lower end is horizontal. Therefore when the condyles are placed horizontally on a flat surface, the angle between the shaft and the horizontal plane is more in males (800) and less in females (760).
Angle of the neck on the shaft (collo-diaphyseal angle) was less in males (<400) and more in females (>500).
Evidence of pregnancy from skeleton
Child birth can cause certain changes in the pelvis especially pubic (pubic scars caused by trauma to ligaments).
Estimation of Stature
When the full Skelton is available direct measurement of the correctly assembled bones with allowances given to the length of missing intervertebral discs and soft tissue thickness of scalp and heel and the thickness of the joint cartilage would give you an approximate measurement.
When the full skeleton is not available the long bones can be used to estimate the stature. The best is femur then tibia, humerus and radius in descending order. The length of the bone taken using a osteometric boards should be entered into one of the formulas, which give the estimated stature of the person e.g. REFERENCE: Jantz, R. L., "Modification of the Trotter and Gieser Female Stature Estimation Formulae" Journal of Forensic Sciences, JFSCA, Vol. 37, No. 5, September 1992, pp. 1230-1235. (http://library-resources.cqu.edu.au/JFS/PDF/vol_37/iss_5/JFS375921230.pdf)
Fig. 09. Osteometric Board
Estimation of the Age
Methods used in the estimation of the ‘skeletal’ age differ with the ‘age group’ to which the skeleton belongs. For instance the methods used in fetal bones cannot be used in estimation of a skeleton of a middle aged man.
The fetus and young infant
The appearance of ossification centres is the most important ageing criterion in this age group. All the bones except the cranial bones are formed in cartilage. Then they ossify from one or more places with appearance of ossification centres, which happens according to a set pattern and time. If there is a bone with an ossification centre already appeared we know that it should be more than a certain age. For instance, the ossification centre at the lower end of the femur should appear and more than a centimetre in diameter at term.
However, when a fetus or a young infant is skeletalized these ossification centres are usually dispersed as rest of the cartilaginous bone is destroyed very quickly.
Femoral length is a useful measurement in estimation of age in fetus and young infants.

Fig 10. This shows the ages of appearance of ossification centres in the foot and hand
The child and young adult
The appearance of ossification centres is complete by around 5 years. After that fusion of epiphyses can be used up to about 25 years of age. The medial clavicular epiphysis is usually the last to fuse.

Fig. 11. Fusion of few epiphyses
Skeletal ageing in later years
After the eruption of 3rdmolar and fusion of the epiphysis of the medial end of the clavicle, which happened in the middle of the 3rd decade (around 25 years) we run out of reliable methods to estimate age. After that the skeleton will suffer subtle change without any dramatic occurrences like appearance of ossification centres and fusion of epiphyses. The following methods are based on age related bone changes caused by slow degeneration.
Pubic Symphysis
The changes occur at the opposing faces of two pubic symphysis are used to estimate age from 18 to about 50 years.

Fig.12. Comparison of the face of pubic symphysis. 18 years in the left and the >50 years in the right

Fig.12. Comparison of the face of pubic symphysis. 18 years in the left and the >50 years in the right
Fig 12. Faces of pubic symphysis showing changes of different ages. 18 years at the left and >50 years at the right. These different stages represent a age range.
Sternal Rib
Age related degenerative changes in the costo-chondral junction can also be used to estimate age.
Fig. 13. Sternal end of the rib (usually 4th is used) showing stages of age related degenerative changes. Age is estimated according to set of degenerative changes described under each phase.
Skull Sutures
Skull sutures, which are open in young, will fuse with age. However, it is not considered to be a reliable index of age. However basi-sphenoid synchondrosis (situated at the base of he skull between the sphenoid and foramen magnum) is considered to be much more accurate indicator fusing about 20 years. The suture between two halves of frontal bone,‘metopic suture’, fuses at 2 years.
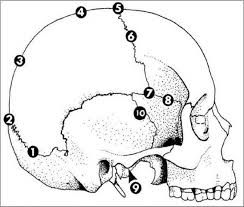
Fig. 14. These different areas of skull sutures fuse at different ages.
Fig. 14. These different areas of skull sutures fuse at different ages.
Radiological method
Radiology can be used to estimation of age. E.g. From internal structure of the cancellous bone and cortical thickness of the head of humerus and femur
Histology
Remodelling of Haversian structure is potential criterion for estimation of age.
Determination of Race from Skeleton
Skeleton especially skull can be used to determine race, Caucasoid, Mongoloid or Negroid. Since Sri Lankans are racially mixed it is not very important in identifying local Skeletal remains.
Personal or Specific Identification from Skeletal Material
After the conclusion of the general identification of the skeletal remains as to the sex, age and stature the examiner should look for any idiosyncratic features which may help in specific identification of the skeleton. As mentioned earlier this is basically an exercise in comparison of post-mortem data, obtained from the examination of the skeletal remains and ante mortem data obtained from the missing person/s, whose remains are suspected to be the remains under investigations.
These features can be two
1. Anatomical shapes and structures can be measured or observed by radiology and other means such as frontal sinus comparison, craniotomy and bone architecture
2. Idiosyncratic features such as healing/healed fractures, surgical prosthesis, bone diseases, congenital defects, amputations etc.
Photo superimposition
This technique involves the superimposition of the photograph of the skull, taken in the same orientation as the photograph, on a photograph of the missing person taken when he/she was alive. Then major anatomical landmarks of the face such as nasion, supraorbital ridges, angle of the jaw, nasal aperture etc is matched. Now it is done using a video camera as well.

Fig. 14. Photo superimposition
Reconstruction of the face from the skull
This technique involves sculpting the face on the skull under examination using modelling clay. To do that the sculpture should know the average tissue thickness over the various anatomical land marks on the face. This is considered to be more of an art than science. Recently computer graphics has been used to reconstruct faces using computers.

Fig. 15. Facial reconstruction
Identification of the dead by dentition
Fig. 15. Facial reconstruction
Identification of the dead by dentition
Since the teeth are the most resistant tissues, which may survive even in severely burned bodies. They are widely used in identification in mass disasters like aviation and natural disasters and tsunami etc. Dental identification is used in different situation in developed countries such as victims of violent crimes, fires, motor vehicle accidents and work place accidents. Sometimes the bodies can be disfigured to such an extent that identification by a family member is neither reliable nor desirable. Even in some developed countries because of the lack of a comprehensive fingerprint database, dental identification continues to be crucial.
Dental identification takes two main forms like in the case of skeletal remains. The first is comparative identification which is the most frequently performed examination. The objective of the examination is to establish that the remains under investigation and a person whose ante mortem dental records are available are the same individual. The second is performed where the ante mortem dental records are not available and a tentative identification of the individual is also not possible by other means. In these cases the forensic dentist will complete a post-mortem dental profile highlighting in the characteristics of the individual which would narrow the search for the ante mortem materials.
The rationale behind the concept of dental identification is that post-mortem dental remains can be compared with ante mortem dental records, including written notes, study casts, radiographs, etc, to confirm identity. It is easier to achieve positive identification of the individuals with complex dental treatments than the ones with little or no restorative treatment.
The ante mortem dental records are usually traced by the police after making tentative or presumptive identification based on personal effects or circumstantial evidence.
The post mortem dental record made by the forensic dentist by careful charting and written descriptions of the dental structures and radiographs will be compared with the ante mortem record.

Fig. 16. A post-mortem dental record
Forensic dentist can assist the anthropologist in determining race, Caucasoid, Mongoloid and Negroid, by dental characteristics, such as cusps of Carabelli, shovel-shaped incisors and multi-cusped premolars. There are no sex differences are apparent in the morphology of teeth. Microscopic examination of teeth can confirm sex by the presence or absence of Y-chromatin and DNA analysis can also reveal sex.
Age estimation
Teeth are formed as soft tissue buds under the epithelial surface of the jaw. Then they are mineralized to form crown initially and roots subsequently. Once the crowns are formed they erupt through the epithelial surface of the jaw. All these stages are used to determine the age of the individual.
Mineralisation
Deciduous teeth commence mineralisation at about 20 weeks of intrauterine life; by 28 weeks all the deciduous teeth have commenced mineralisation. Mineralisation of the anterior buccal cup of the lower first permanent molar commences a week or two before birth. Mineralisation of other teeth commence after birth in a fairly well defined sequence.
Incremental lines
The mineralisation of dental hard tissue occurs in ‘diurnal’ rhythm. This can be seen as a series of periodic lines under the microscope, which are called ‘incremental lines’. These lines vary in character due to variety of reasons. For instance birth is particularly a stressful time due to change of environment and nutrition. The incremental line formed around this time is prominent compared to others and is called‘neonatal line’. This can be seen in each of the deciduous teeth and lower first molar as they are the teeth which have commenced mineralisation at birth.
This can be used to determine whether a child, whose skeletal remains are under investigation, had a live birth and sometimes to determine how long it would have survived after birth if rate of growth of dental hard tissue, enamel and dentine, is known.
Individualized features of the incremental lines can also be used to identify the teeth belong to a single individual in examination of fragmentary human remains.
The accuracy of age estimation from dental examination varies of the age of the dentition as in the case of the bone. During the development of teeth up to about 15 years accuracy of about plus or minus one year should be obtainable. Microscopic examination of incremental pattern of in the teeth may provide an accuracy of plus or minus few days.
After the development of teeth is complete only available methods for age estimation are estimation of progressive‘wear’ and ‘ageing’ process of teeth. The best accuracy achieved by this process is claimed to be plus or minus 10 years.
Age assessment method of the forming dentition
a. Use of charts prepared from population surveys
As already mentioned deciduous dentition commences calcification from two to four months before birth (20-28 weeks in utero). This continuous until the last deciduous tooth, second deciduous molar, is complete at about three and half to four years of age.
The permanent dentition commences mineralisation just before birth, progressively replaces the deciduous dentition from seven to 15 years, and it itself complete by 20 – 25 years of age.
Therefore, at anytime up to the end of the second decade the jaw contain one or more partly formed teeth. The state of development forming teeth reflects the age of the individual. Therefore age estimation is made by the examination of the degree of tooth formation of all the teeth of the jaw.
In practice jaws are radiographed and the state of development of the whole dentition is compared with the stages shown on standard charts. They are based on dental surveys of cross sections of the population.

b.) Age estimation from the weight of the development dentition
This is done by progressive increase in weight of the growing dental tissue.
First identify the ‘neonatal’ line and the count the incremental lines from it to the edge of forming enamel front. It is assumed that each increment represents one day’s addition of enamel.
D.) Eruption of Teeth
Eruption dates of the teeth are highly variable and the actual developmental stages of the teeth are more accurate. Third molar development is used by some forensic dentists to assign age to young adults.

Fig. 18. Eruption chart
Fig. 18. Eruption chart
Age assessment methods applied to the adult dentition
At the end of the tooth formation, usually about 20-22 years of age, stages of tooth development are no longer applied. In the adult dentition age estimation is done by the assessment of the progression of ‘wear’ and ‘age’ changes in teeth.
Gustafson (1950) used six progressive changes after giving a score from a scale of 0-3 to each in his method of estimation of age.
The six criteria he used are
1. Crown Attrition
2. Secondary dentition deposition
3. Apical migration of periodontal membrane attachment
4. Root transparency
5. Root resorbtion
Comparative techniques
Dental Radiographs
Positive identification can be achieved by comparing the post-mortem dental radiographs with ante mortem photograph. The following features can be used
1. Tooth shape
Congenital and acquired defects such as peg-shaped teeth, ‘dens-in-dente’, hypoplastic defects
2. Caries and periodontal disease
Since they are progressive a recent ante mortem radiograph is needed for comparison. The treatment given to dental caries such as fillings, bridging etc. can also be used.
3. Root treatment
4. Extraction sockets
5. Impacted and unerupted teeth
6. Fractures
They can occur sometime before death, in the course of an assault leading to depth, at the time of death (aircraft accident), after death.
7. Pathology
e.g. haemangioma, Paget’s disease, fibrous dysplasia, neoplasia etc.
Identification of the Living
Sometimes the doctors are requested to do certain aspect of identification on living persons. The most common scenario is to estimate the age of person who does not have a birth certificate to apply for the identity card. Sometimes child victims of abuse may also need to estimation of age as they do not have birth certificates. The same techniques described under the identification of skeletal remains are used in these instances. Radiology is used to look at the ossification centres and fusion of epiphyses. Dentist’s expertise is also sought to estimate age by dentition. When these people are referred to radiology they take an x-ray of the left hand and wrist and compare the fusion of epiphysis by referring to an atlas called Greulich and Pyle atlas.

Fig.19. Example of how to use Greulich and Pyle atlas
Fig.19. Example of how to use Greulich and Pyle atlas
Priyanjith Perera
30 November 2012
30 November 2012
No comments:
Post a Comment